|
Cracking the Navicular Code 
Navicular syndrome is one of the most common causes of fore limb lameness in performance horses. Several years ago, most of us thought that all horses with navicular syndrome had relatively the same problem; inflammation in and around the navicular bone. The advent of new diagnostic imaging modalities, particularly Magnetic Resonance Imaging (or MRI), has revealed a multitude of potential forms of pathology that can occur within this region. This knowledge has not only changed the way that we work-up these cases� it has also enabled veterinarians to streamline their approach to treatment.
Pathology associated with the following structures can causes clinical signs of navicular syndrome: |
 |
-
Navicular Bone
-
Navicular Bursa
-
Collateral Sesamoidean Ligament
-
Distal Sesamoidean Impar Ligament
-
Distal Digital Annular Ligament
-
Distal Palmar Digital (PD) Sheath
-
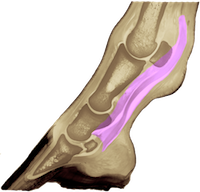
Deep Digital Flexor Tendon
|
-
Laminae
-
Distal Interphalangeal (DIP) or Coffin Joint
-
Collateral Ligaments of Coffin Joint
-
Third Phalanx (Coffin Bone or P3)
-
Collateral Ligaments of Pastern Joint
-
Proximal Interphalangeal (PIP) or Pastern Joint
-
Second Phalanx (Short Pastern Bone or P2)
-
Distal First Phalanx (Long Pastern Bone or P1)
-
Straight Sesamoidean Ligament
-
Obliqued Sesamoidean Ligaments
-
Palmar Fetlock Joint
|
With all of these potential causes of palmar foot pain how do we examine horses with the intention of arriving at a specific diagnosis
Here is a strategy typically implemented at The Atlanta Equine Clinic: |
HISTORY |
The horse usually presents with a history of bilateral forelimb lameness of varying duration. Since foot pain generally generates a weightbearing lameness, most clients complain of a “head bob", which is usually worse when traveling with the affected limb on the inside of a circle. The trot tends to the be the worst gait. |
 |
CLINICAL EVALUATION |
Passive Examination |
The horse may have one or two high/ contracted fore feet. In many cases, a response can be elicited during hoof testing along the frog. |
Active Examination |
The horse typically exhibits weightbearing lameness in one or (more commonly) both fore feet. Lameness is usually accentuated with the affected limb on the inside of a circle and when trotting on a hard surface. In some cases, a positive response to digital extension is demonstrable. |
Perineural Anesthesia |
In cases of navicular syndrome, the horse's soundness will typically improve 85% or more with local palmar digital (PD) perineural anesthesia. If less than 85% improvement is observed pursuant to this block, then alternate sources of lameness (other than navicular syndrome) are investigated. |
|
1. Anesthetize (block) or Empirically Treat Coffin Joint |
 |
2. Anesthetize (block) or Empirically Treat Palmar Digital Sheath |
|
3. Anesthetize (block) or Empirically Treat Navicular Bursa |
 |
|
|
 |
 |
 |
Possible sources include the coffin joint, the DIP collateral ligaments, proximal P3, distal P2, the collateral sesamoidean ligaments, the distal sesamoidean impar ligament, the dorsal aspect of the navicular bone, and eventually the navicular bursa (if given enough time). |
Possible sources include the superficial digital flexor tendon branches, the proximal aspect of the deep digital flexor tendon, the straight sesamoidean ligament, the obliqued sesamoidean ligaments, the T-ligament and the distal digital annular ligament. |
Possible sources include the navicular bursa, the insertion of the deep digital flexor tendon onto P3, the apposition of the deep digital flexor tendon and navicular bone, the flexor surface of the navicular bone, the collateral sesamoidean ligaments, the distal sesamoidean impar ligament and the T-ligament. |
Further Diagnostic Options: Radiographic, ultrasonographic and/or MR imaging. |
Further Diagnostic Options: Ultrasonographic and/or MR imaging. |
Further Diagnostic Options: Radiographic, ultrasonographic and/or MR imaging. |
Treatment Options: Rest, corrective shoeing, aspirin, isoxuprine, coffin joint injection, arthroscopic surgery and/or palmar digital (PD) neurectomy.
*PD neurectomy is reserved for severe cases that are refractory to other forms of therapy and those in which significant compromise of the DIP collateral ligaments is not appreciated). |
Treatment Options: Rest, corrective shoeing, intrathecal injection, intralesional injection (stem cells), ESWT, and/or tenoscopic surgery.
*Palmar digital (PD) neurectomy is not recommended in these cases. |
Treatment Options: Rest, corrective shoeing, aspirin, isoxuprine, injection of the navicular bursa, ESWT, bursoscopic surgery and/or palmar digital (PD) neurectomy.
*PD neurectomy is reserved for severe cases that are refractory to other forms of therapy and those in which excessive erosion of the flexor surface of the navicular bone and/or significant compromise of the DDFT is not appreciated). |
|
